The Use of TISSEEL [Fibrin Sealant] in Complex Gynecologic Surgery
O.R. Insights Blog
The Use of TISSEEL [Fibrin Sealant] in Complex Gynecologic Surgery
Many techniques and materials are available to achieve hemostasis during gynecologic surgery.1 Sutures, hemoclips, and electrocautery are predominantly used, but in situations in which these methods alone are insufficient, topical hemostatic agents can serve as an alternative option to reduce thermal damage, devascularization, and tissue necrosis while also reducing blood loss.1,2 There are many hemostatic products available today, including fibrin sealants, which are utilized for hemostasis and tissue sealing across a range of surgical procedures, including gynecologic surgery.1
Complex gynecologic surgeries demand advanced techniques and meticulous planning. In this blog, Dwight D. Im, MD, FACOG,† a renowned board-certified gynecologic surgeon and leader of the prestigious gynecology and robotic surgery programs at Mercy Medical Center in Baltimore, provides an overview of his systematic approach to navigating challenging pelvic anatomy. Effective hemostasis is a cornerstone of success in these procedures, and Dr. Im relies on fibrin sealant to achieve it.3
Introduction
Bleeding can be a complication of surgery that may lead to substantial morbidity and mortality.4 Specifically, 7.5% of US gynecologic patients will experience bleeding-related complications and/or blood transfusions that can increase length of stay, mortality, and resource utilization.4 Notably, among adults who had an inpatient gynecologic procedure during 2006–2007, patients with bleeding-related complications had statistically significantly higher average costs ($9,295) relative to patients without complications ($6,490), thus leading to additional costs of up to $2,805.4
Moreover, gynecologic surgery can present a wide range of bleeding types, ranging from mild capillary-like oozing across broad surfaces to life threatening spurting or gushing.5,6 A surgeon-validated scale, known as the Validated Intraoperative Bleeding Scale (i.e., VIBe SCALE tool), is graded on a 5-point scale from 0 (no bleeding) to 4 (life threatening).5,6 The VIBe SCALE tool provides a standardized, reproducible method for evaluating bleeding severity and is available to help guide surgical teams in the evaluation of bleeding severity in open surgical procedure and to ultimately choose an appropriate agent for effective hemostasis.5,6
7.5% of US gynecologic patients
will have bleeding-related complications and/or blood transfusions that can increase length of stay, mortality and resource utilization.4
Bleeding related complications
may lead to additional costs of up to $2,805 in reproductive surgery patients relative to patients without complications.4
Gynecologic surgery
can present bleeding challenges throughout the duration of the procedure, ranging from mild capillary-like oozing across broad surfaces to life threatening spurting or gushing.5,6
Hemostasis can be a particularly challenging problem
laparoscopically as intracorporeal suturing may be too slow or cumbersome.7
During surgical procedures, bleeding control may be difficult or ineffective.7 A potential solution is the use of adjunct topical hemostatic agents to address these challenges in complex gynecologic surgery, such as laparoscopic excision of endometriomas.7
I don't know where I am.
How do I get to where I need to go?
Overview of Complex Gynecologic Surgery
In my experience, several factors can contribute to the complexity of hysterectomy and other gynecologic surgeries. These factors include inadequate exposure, difficult dissection, pelvic adhesive disease, retroperitoneal fibrosis, and presence of fibroids and pelvic adhesions. Notably, the size and location of fibroids greatly influence the complexity of hysterectomies and other gynecologic surgeries.
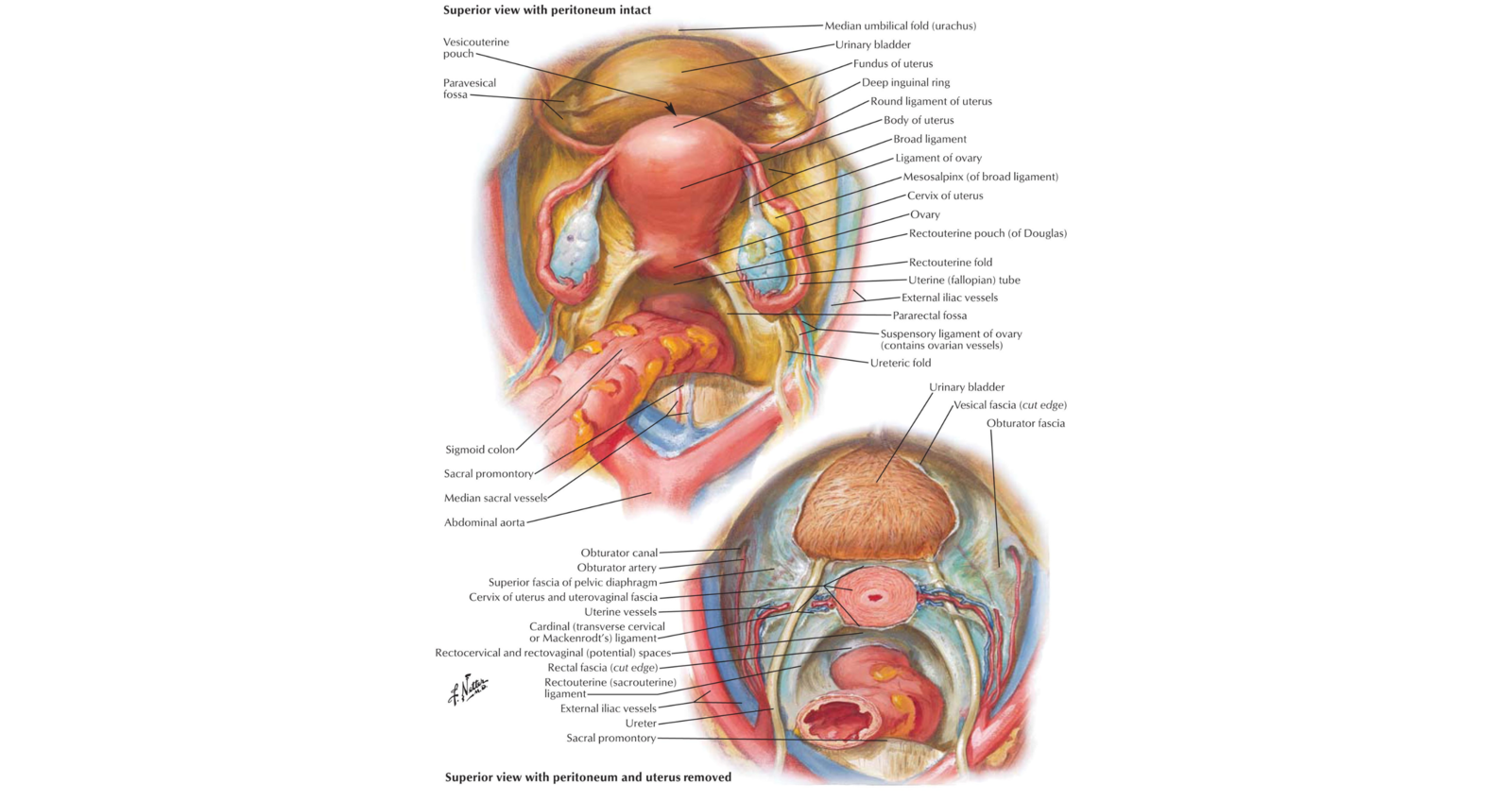
Insufficient visualization of the surgical field significantly hinders the procedure and challenging anatomical planes make precise dissection difficult. Below is a diagram of the pelvic anatomy, showing connective tissue planes and spaces of the female pelvis and a diagrammatic cross section of the female pelvis through the cervix (Figure 1). The avascular spaces of the female pelvis include prevesical, vesicovaginal, rectovaginal, retrorectal, paravesical, and pararectal spaces.8
Specifically, regarding the challenges of accessing the pararectal space, I would also add that it's a challenging area to develop, requiring careful consideration of several anatomical elements. Successfully accessing and operating in this region may be accomplished as described in my IMSWAY technique.
My IMSWAY technique provides a systematic and reproducible method for accessing the retroperitoneal space during complex hysterectomy, particularly when involving fibroids. The steps involve:
- Infundibulopelvic ligament (IP)
- Medial leaf of peritoneum
- Skeletonize ureter
- Water under the bridge
- At origin of uterine artery
- Yes! A Success!
All pelvic surgery starts with the IP ligament. Identifying and skeletonizing the IP ligament is the foundation of the approach. To skeletonize the ureter, use the IP ligament to help locate and gently dissect the ureter off the medial leaf of the peritoneum. Ensure dissection is lateral to the ureter, while staying close to the ureter. Follow the ureter to the “tunnel” via the vesicouterine ligament and use the ureter as a guide to locate the internal iliac artery and uterine artery/vein in the pararectal space. Then we move into water under the bridge. This refers to the area where the uterine artery crosses anterior to the ureter. Careful dissection around the uterine artery, along with dissection of the hypogastric artery, expands access to the pararectal space. Finally, once the pararectal space is adequately developed, clamp, coagulate, and/or cut the uterine artery at its origin. Securing the uterine artery in this final step helps minimize the bleeding.
Bleeding control may be difficult or ineffective in differing surgical procedures and approaches.7 Thus, securing hemostasis can be a challenge,7 but many techniques, materials, and hemostatic agents are available to achieve hemostasis during gynecologic surgery.1 Sutures, hemoclips, and electrocautery are predominantly used, but in situations in which these methods alone are insufficient, topical hemostatic agents may be useful adjuncts for achieving hemostatis.1,2,3,7 Many types of topical hemostatic agents are available today, including fibrin sealants, which are utilized for hemostasis across a range of surgical procedures, including gynecologic surgery.1,3
Introduction to Tisseel [fibrin sealant]
TISSEEL [Fibrin Sealant] Indication
Tisseel [fibrin sealant] is indicated for use as an adjunct to hemostasis in adult and pediatric patients (>1 month of age) undergoing surgery when control of bleeding by conventional surgical techniques (such as suture, ligature, and cautery) is ineffective or impractical.3 Tisseel [fibrin sealant] is effective in heparinized patients and is also indicated as an adjunct to standard surgical techniques (such as suture and ligature) to prevent leakage from colonic anastomoses following the reversal of temporary colostomies.3
Composition of TISSEEL [Fibrin Sealant]
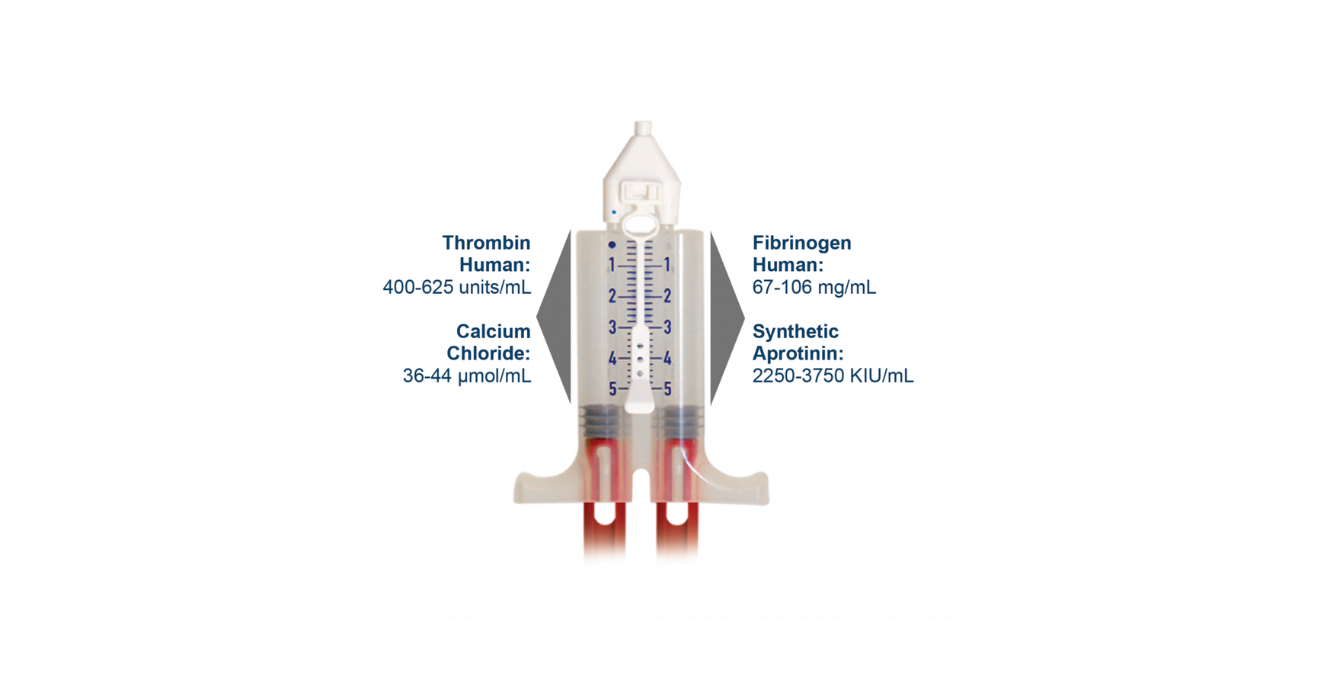
Tisseel [fibrin sealant] is a two-component fibrin sealant made from pooled human plasma.3 When combined, the two components, a human sealer protein and human thrombin mimic the final stage of the blood coagulation cascade.3 The sealer protein is a sterile, non-pyrogenic, vapor heated and solvent/detergent treated preparation made from pooled human plasma. The sealer protein also contains a fibrinolysis inhibitor, aprotinin, that is synthetic and completely of non-human/non-animal origin.3 The thrombin is also a sterile, non-pyrogenic, vapor heated and solvent/detergent treated preparation made from pooled human plasma. In the presence of small amounts of calcium and Factor XIII, the thrombin converts fibrinogen into insoluble fibrin, the final stable form of the agent.3 Details of the composition of Tisseel [fibrin sealant] are provided in Figure 2.3
Figure 2: Tisseel [fibrin sealant] Composition: Dual-Chambered Syringe3
How TISSEEL [Fibrin Sealant] Works
Upon mixing the human sealer protein and thrombin, soluble fibrinogen is transformed into fibrin, forming a rubber-like mass that adheres to the wound surface and achieves hemostasis and sealing or gluing of tissues.3 Tisseel [fibrin sealant] mimics the final coagulation cascade step as it has all relevant components to form a clot.3 Thrombin is a highly specific protease that transforms the fibrinogen contained in Sealer Protein into fibrin. Fibrinolysis inhibitor, aprotinin (synthetic), is a polyvalent protease inhibitor that prevents premature degradation of fibrin. Preclinical studies have shown that incorporation of aprotinin increases resistance of the fibrin sealant clot to degradation in a fibrinolytic environment.3
Formation of a Physiologic Clot
When comparing scanning electron microscope (x10,000) images of the clot formed by Tisseel [fibrin sealant] as compared to a physiologic clot, the clot formed by Tisseel [fibrin sealant] closely resembles a physiologic clot (Figure 3).9-11
Figure 3: Comparison of Fibrin Clot with a Physiologic Clot9-12
Scanning electron microscope (SEM) images

Normal Physiologic Clot
An open-pore structure enables diffusion of nutrients, stem cells, an in-growth fibroblasts which helps promote the body’s natural wound-healing process.
![Tisseel [fibrin sealant] Clot x10,000](/sites/g/files/ebysai4111/files/2025-04/Figure-3-Tisseel.png)
TISSEEL [fibrin sealant] Clot
Tisseel [fibrin sealant] shows a clot structure that closely resembles a normal physiologic clot.
The Use of TISSEEL [fibrin sealant] in Complex Gynecologic Surgery: Case Studies
The use of Tisseel [fibrin sealant] has demonstrated benefits in reducing bleeding in complex gynecologic surgeries.13 Below we present two case studies of patients who received Tisseel [fibrin sealant] for adjunctive hemostasis.
Selected Risk Information for Tisseel (fibrin sealant): Do not use where the minimum recommended distance from the applicator tip to the target site cannot be reassured. Please see full IRI and link to Prescribing Information to follow.
Video 1. Complex Gynecologic Surgery: Case Study 1
A 51-year-old patient presented with abdominal bloating and pelvic pain. Pelvic sonography revealed a solid uterine mass, measuring 10.6 x 9.9 x 6.8 cm. The operation employed use of the IMSWAY technique, vasopressin, and a single tooth tenaculum. Tisseel [fibrin sealant] was used for adjunctive hemostasis.
Video 2. Complex Gynecologic Surgery: Case Study 2
A 44-year-old patient with fibroids and abnormal uterine bleeding underwent pelvic magnetic resonance imaging (MRI). The MRI showed presence of multiple intramural fibroids of varying sizes: one measuring 3.8 x 3.6 x 3.6 cm, another 3.1 x 3.6 x 3.2 cm in the anterior fundus, and a smaller one measuring 2.1 x 2.1 x 2.0 cm. Additionally, a complex heterogeneous mass of 11.8 x 8.9 x 7.1 cm was found in the right adnexa. The surgical strategy in this case included the use of vasopressin, a single-tooth tenaculum, and the IMSWAY technique. Tisseel [fibrin sealant] was used for adjunctive hemostasis.
Summary
In my experience, complex hysterectomies, especially those involving fibroids, demand meticulous attention to detail. Successfully navigating challenging pelvic anatomy requires a systematic approach, and I have found that beginning with precise identification and skeletonization of the IP ligament is key. My IMSWAY technique provides a reproducible method for accessing the retroperitoneal space, crucial for managing situations where fibroids present significant challenges. Using vasopressin and a single-tooth tenaculum (for traction) aid in exposure during the gynecological procedures as well.
Effective hemostasis is paramount for successful and efficient surgery. While sutures, hemoclips, and electrocautery are predominantly used, in complex cases where bleeding is more significant or challenging, a topical hemostatic agent can be an invaluable adjunct.1,2,3 In my practice, we utilize Tisseel [fibrin sealant] to manage generalized oozing, finding it particularly effective in these situations. The case studies presented, along with video demonstrations, showcase the practical application of these techniques and highlight the effectiveness of Tisseel [fibrin sealant] in managing surgical bleeding. Combining precise surgical technique (IMSWAY) with an appropriate adjunctive hemostatic agent supports surgeons in achieving the surgical outcomes they desire with complex gynecologic procedures.
*Dr. Im was compensated for his time developing the content for this blog.
Indications and Important Risk Information for TISSEEL [fibrin sealant]
TISSEEL [Fibrin Sealant] Indications
Hemostasis: Tisseel [fibrin sealant] is a fibrin sealant indicated for use as an adjunct to hemostasis in adult and pediatric patients (> 1 month of age) undergoing surgery when control of bleeding by conventional surgical techniques (such as suture, ligature, and cautery) is ineffective or impractical. Tisseel [fibrin sealant] is effective in heparinized patients.
Sealing: Tisseel [fibrin sealant] is a fibrin sealant indicated as an adjunct to standard surgical techniques (such as suture and ligature) to prevent leakage from colonic anastomoses following the reversal of temporary colostomies.
Important Risk Information for TISSEEL [fibrin sealant]
For Topical Use Only. Do not inject TISSEEL [fibrin sealant] directly into the circulatory system or into highly vascularized tissue. Intravascular application of TISSEEL [fibrin sealant] can lead to intravascular coagulation, can result in life- threatening thromboembolic events, and can increase the likelihood and severity of acute hypersensitivity reactions in susceptible patients. To minimize the risk of intravascular application, exercise caution when using Tisseel [fibrin sealant] in surgery.
Do not use Tisseel [fibrin sealant] in individuals with a known hypersensitivity to aprotinin.
Do not use Tisseel [fibrin sealant] for treatment of severe or brisk arterial or venous bleeding. In these situations, Tisseel [fibrin sealant] will be washed away in the flow of blood before hemostasis can be attained.
Do not spray Tisseel [fibrin sealant] where the minimum recommended distance from the applicator tip to the target site cannot be assured.
Hypersensitivity or allergic/anaphylactoid reactions can occur with the use of Tisseel [fibrin sealant]. Such reactions may especially be seen if Tisseel [fibrin sealant] is applied repeatedly over time or in the same setting, or if systemic aprotinin has been administered previously.
Aprotinin is known to be associated with anaphylactic reactions. Even in the case of strict local application of aprotinin, there is a risk of anaphylactic reactions to aprotinin, particularly in the case of previous exposure.
Discontinue administration of Tisseel [fibrin sealant] in the event of hypersensitivity reactions. Remove remaining product from the application site.
Air or gas embolism has occurred when fibrin sealant was administered using pressurized gas. This can occur if a spray device is used at higher than recommended pressures and in closer than recommended proximity to the tissue surface.
When using the EasySpray device, or an equivalent spray device for open surgical procedures cleared by FDA, Tisseel [fibrin sealant] must not be sprayed in enclosed body areas and must be sprayed onto only visible application sites.
Tisseel [fibrin sealant] is denatured when exposing to solutions containing alcohol, iodine or heavy metals. If any of these substances have been used to clean the wound area, the area must be thoroughly rinsed before the application of Tisseel [fibrin sealant].
Apply Tisseel [fibrin sealant] as a thin layer by dripping or spraying using cannula or spray set. Excess clot thickness can negatively interfere with wound healing.
The safety and effectiveness of Tisseel [fibrin sealant] used alone or in combination with biocompatible carriers in neurosurgical procedures or other surgeries involving confined spaces have not been evaluated; its use in this setting is not FDA approved.
Tisseel [fibrin sealant] is made from human plasma. It may carry a risk of transmitting infectious agents, e.g., viruses, the variant Creutzfeldt-Jakob disease (vCJD) agent and, theoretically, the Creutzfeldt-Jakob disease (CJD) agent.
Please see accompanying full Prescribing Information: http://baxterpi.com/pi-pdf/Tisseel_PI.pdf
Baxter, EasySpray and Tisseel are registered trademarks of Baxter International Inc. or its subsidiaries.